

No Longer Hip
Author: Sean Aubuchon, MD
Peer-Reviewer: Justine Ko, MD, CAQ-SM
Final Editor: Alex Tomesch, MD, CAQ-SM
A 77-year-old female with past medical history significant for Parkinson’s disease and hypertension presents to the ED after a mechanical fall upon getting into bed. Since that time, she has endorsed left hip pain and inability to ambulate.


Image 1 and 2. Plain radiographs of the patient’s left hip. Author’s own images.
Which imaging modalities can be used? Is there a role for other diagnostic modalities such as ultrasound?
Radiographs are the gold standard imaging modality. Recommended views include an AP pelvis, AP hip, cross table lateral, and a full length femur film [2]. CT and MRI are typically not indicated, but due to their high specificity can be used when there is high clinical suspicion and initial films are negative.
Ultrasound (Image 3 & 4), however, may offer an accurate means for diagnosis. Though sensitivities and specificities of ultrasound in diagnosis of femur fractures have not been well described, some authors have attempted to explore its utility. Bozorgia et al. found that ultrasound has a 90% sensitivity for detecting femur shaft fractures in adults [4]. The benefit of ultrasound is that it can rapidly be incorporated into a physician’s initial evaluation of a patient, potentially reduce the necessity of painful manipulation required by radiographs, and allow for simultaneous evaluation for ultrasound-guided regional nerve blocks.
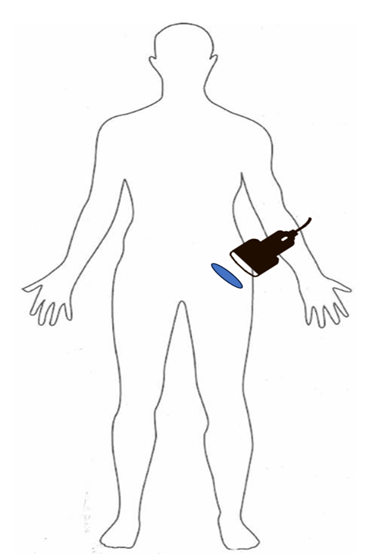
Figure 1. Suggested initial orientation of the ultrasound probe to evaluate the femoral neck and proximal femur. Author’s own image
Image 3 and 4. Linear (top) and curvilinear (bottom) ultrasound show a cortical irregularity (blue arrow) at the level of the femoral neck/intertrochanteric femur. Author’s own images.
References
[1] Emmerson BR, Varacallo M, Inman D. Hip Fracture Overview. InStatPearls [Internet] 2023 Aug 08. StatPearls Publishing.Available;https://
[2] Attum, B., & Pilson, H. Intertrochanteric Femur Fracture. In StatPearls [Internet] 2023 Aug 08. StatPearls
[3] Zuckerman J. D. (1996). Hip fracture. The New England journal of medicine, 334(23), 1519–1525. https://doi.org/10.1056/
[4 ]Bozorgia, F., Azarb, M. S., Heidaria, S. F., & Khalilianc, A. (2017). Accuracy of Ultrasound for Diagnosis of Femur Bone Fractures in Traumatic Patients. Journal of Clinical & Experimental Orthopaedics, 3(1:27). https://doi.org/10.4172/2471-
[5] Handoll, H. H., Queally, J. M., & Parker, M. J. (2011). Pre-operative traction for hip fractures in adults. The Cochrane database of systematic reviews, (12), CD000168. https://doi.org/10.1002/
[6] Girón-Arango, L., Peng, P. W. H., Chin, K. J., Brull, R., & Perlas, A. (2018). Pericapsular Nerve Group (PENG) Block for Hip Fracture. Regional anesthesia and pain medicine, 43(8), 859–863. https://doi.org/10.1097/AAP.
[7] Chlebeck, J. D., Birch, C. E., Blankstein, M., Kristiansen, T., Bartlett, C. S., & Schottel, P. C. (2019). Nonoperative Geriatric Hip Fracture Treatment Is Associated With Increased Mortality: A Matched Cohort Study. Journal of orthopaedic trauma, 33(7), 346–350. https://doi.org/10.1097/BOT.
[8] Fischer, H., Maleitzke, T., Eder, C., Ahmad, S., Stöckle, U., & Braun, K. F. (2021). Management of proximal femur fractures in the elderly: current concepts and treatment options. European journal of medical research, 26(1), 86. https://doi.org/10.1186/