
- Details
- Hits: 379

Regional Anesthesia Interscalene Block
January 2025
Final Reviewer: Justine Ko, MD, CAQ-SM
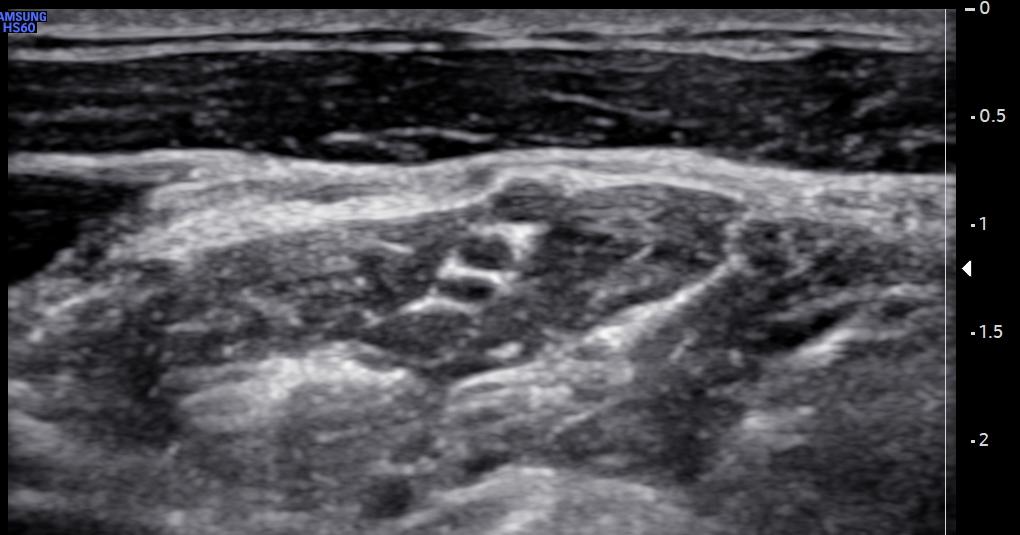
Image 1: Author’s own image.
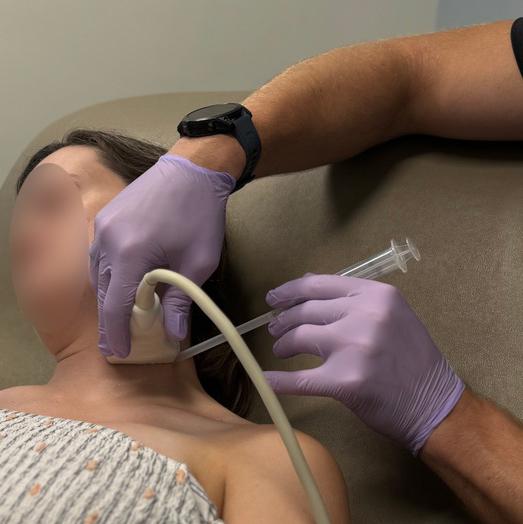
Image 2: Demonstration of the ultrasound technique for this case. Author’s own image.

A 27-year-old male presents with left shoulder pain after falling down a flight of stairs and trying to grab onto a railing to catch himself. He has an obvious deformity to his left shoulder, and is holding his arm in abduction and internal rotation.

Image 4: Left Shoulder Anteroinferior Dislocation, Author’s own image.
What is the distribution of anesthesia for an interscalene nerve block and how does it differ from the supraclavicular nerve block?
The interscalene block targets the nerve roots of C5, C6, and C7 as they pass between the anterior and middle scalene muscles. This occurs before the nerve roots merge to form the superior, middle, and inferior trunks of the brachial plexus, where the supraclavicular block is typically performed. The innervation of the shoulder joint capsule and the bones of the glenohumeral joint is mainly provided by the suprascapular nerve (C5-C6), along with the lateral pectoral nerve (C5-C7) and the axillary nerve (C5-C6). The suprascapular nerve usually branches off before the trunks form, making the interscalene block a better choice for shoulder analgesia. However, the interscalene block is not reliable for achieving blockade of C8, which makes the supraclavicular block a better option for structures innervated by the ulnar nerve (C8-T1). The supraclavicular block is also more reliable in achieving analgesia for pathology in the forearm and hand.

Image 5. Regional anesthesia distribution of the interscalene nerve block, Author’s own image.
You decide to perform an interscalene nerve block to facilitate shoulder reduction and pain control.
What is the patient positioning and positioning of the ultrasound for this procedure?
Like the supraclavicular block, the interscalene block can be performed with the patient either sitting up, partially reclined, or supine. The author prefers to perform it with the patient sitting up, with the operator approaching from a posterolateral position. The ultrasound should be placed across from the operator’s field of view.

How can you identify the desired location for the interscalene nerve block? What are key structures to identify?
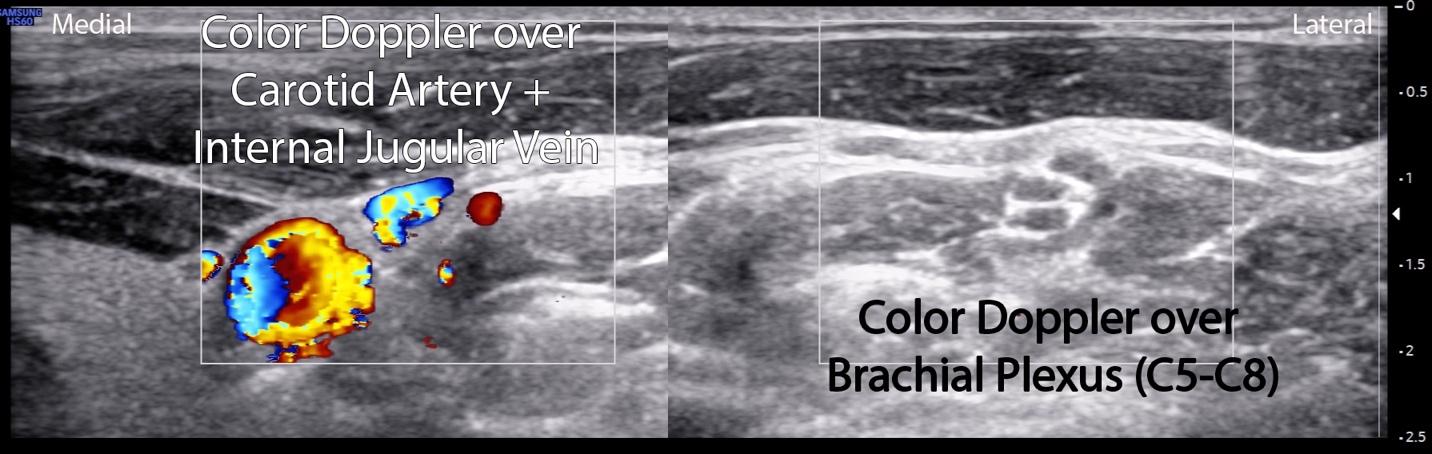
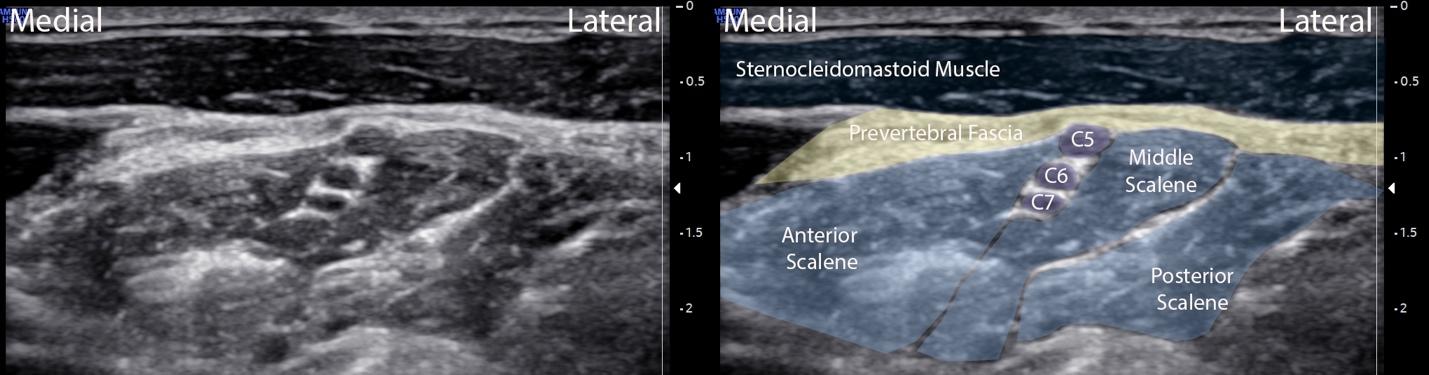
We recommend using the “track-back” method to identify the interscalene space. Start with the linear transducer in the supraclavicular space, in a roughly transverse position just above the clavicle. Identify the brachial plexus lateral and superficial to the subclavian artery. Slide the probe cephalad, tracing the brachial plexus until it splits into three bundles, the C5-C6-C7 nerve roots. This forms a “stoplight” between the anterior and middle scalene muscles. This stoplight is the desired location for the block. Identify the prevertebral fascia, which is superficial to the brachial plexus. Slide the probe medially to identify the carotid artery and internal jugular vein. You can utilize Color Doppler ultrasound to confirm these structures and the brachial plexus location.


What is the target for your needle for the block?
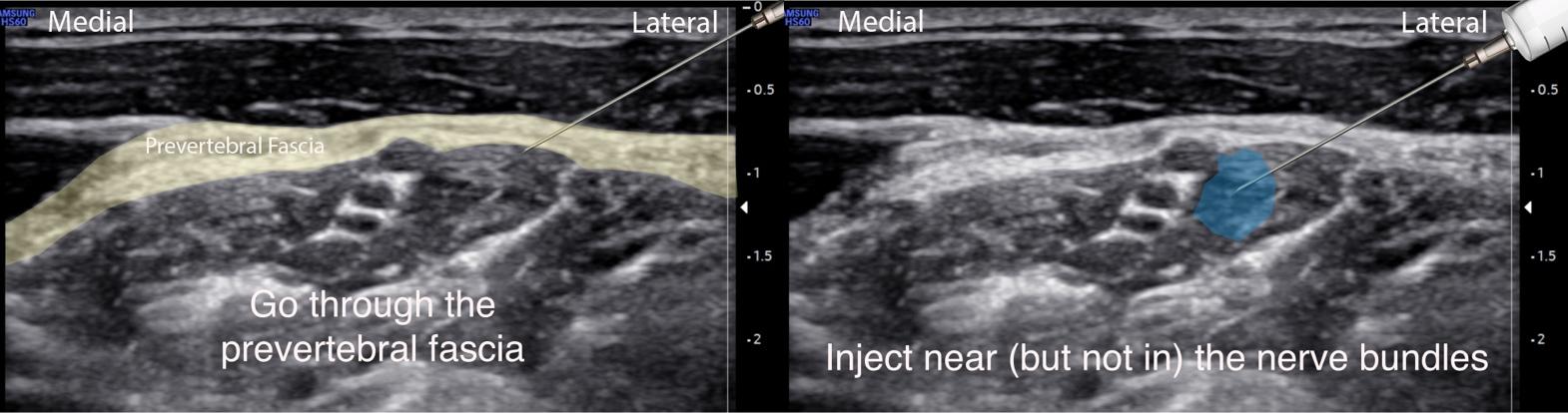
Image 10. Interscalene nerve injection, Author’s own image
References:
[1] Blaivas M, Adhikari S, Lander L. A prospective comparison of procedural sedation and ultrasound-guided interscalene nerve block for shoulder reduction in the emergency department. Acad Emerg Med Off J Soc Acad Emerg Med. 2011;18(9):922-927. doi:10.1111/j.1553-2712.2011.
[2] Raeyat Doost E, Heiran MM, Movahedi M, Mirafzal A. Ultrasound-guided interscalene nerve block vs procedural sedation by propofol and fentanyl for anterior shoulder dislocations. Am J Emerg Med. 2017;35(10):1435-1439. doi:10.1016/j.ajem.2017.04.032
[3] Kreutziger J, Hirschi D, Fischer S, Herzog RF, Zbinden S, Honigmann P. Comparison of interscalene block, general anesthesia, and intravenous analgesia for out-patient shoulder reduction. J Anesth. 2019;33(2):279-286. doi:10.1007/s00540-019-02624-6
[4] Schubert A-K, Dinges H-C, Wulf H, Wiesmann T. Interscalene versus supraclavicular plexus block for the prevention of postoperative pain after shoulder surgery: A systematic review and meta-analysis. Eur J Anaesthesiol. 2019;36(6):427-435. doi:10.1097/EJA.